
The Milky Tooth ©
Why are we encouraged to swallow a toxin?

There was once a Hampshire farmer (Edgar Wilfred Borrow, 1902 – 1990) who had an urge to stop tooth decay in young children even though his honorary doctorate from the University of Louisiana granted in 1983 was in neither dentistry nor in human biology. He learned about the fluoridation of milk in the mid-1900s and became an enthusiastic supporter of the practice. Since it didn’t affect entire communities – just small children – he thought that it was justifiable to add fluoride to school milk to prevent tooth decay.
Had he connected “fluoride” with “fluorine gas” he might not have been so gung-ho about exposing small children to the element.
Dr Edgar Borrow, 1902-1990
Credit: Amazon - Out of print
Early research studies appeared to support the practice as being effective at preventing dental decay but many were poorly designed and of limited or low to moderate quality. (See the Footnote).
Richard Sauerheber investigated the theory of fluoride being transported from the small intestine to our salivary glands. He was sceptical about the claims about fluoride in saliva strengthening tooth surfaces and found that a mere 0.02 ppm fluoride per litre saliva is excreted into the buccal cavity – too little to have any anti-cariogenic effect on teeth. Also, since it’s a bactericide, it knocks out beneficial bacteria in saliva and in the mouth which work hard to stop tooth decay and convert dietary nitrates into nitrites.
Dr Borrow formed the Borrow Foundation in 1971 and appointed Trustees to manage its work and finances. One of his Trustees was and is Andrew Rugg-Gunn, an emeritus professor at Newcastle University. He was a co-founder of the University’s Human Nutrition Research Centre. His list of publications is very long and many of his papers dealt with fluoride present in our diet.
Since its foundation, several developing countries have become involved in giving primary school children fluoridated milk. There was also a time in the years between 2000 and 2018, when some cities and towns in England encouraged their primary schools to provide fluoridated milk. The majority ceased prior to 2019 but Blackpool Borough continues to this day.
A carton of fluoridated milk. Photo by author
The current Director of Public Health for the Borough, Dr Arif Rajpura, is strongly in favour of “dental” milk and has a proactive programme to increase the number of schools offering the milk to pupils.

Dr Arif Rajpura courtesy of Lancs Live
Apparently, this is an “opt out” scheme and parents have to voice their refusal otherwise the child is provided with fluoridated milk.
The fluoride in the milk cartons is minimally (11%) in the form of calcium fluoride whilst the majority remains unbound, allowing fluoride to deposit in bones and teeth as well as in organs. If those tissues are the developing teeth buds, then the fluoride bonds with the immature enamel matrix, thus allegedly fortifying it against tooth decay. The “proof” that it works is recorded at ages five and twelve by dental health researchers when there are less cavities compared to children who drink normal school milk. Research focuses on demonstrating the anti-cariogenic nature of fluoride. However, the mechanism by which fluoride strengthens enamel against bacterial attack is poorly understood. Also, could it be that fluoride is disabling cariogenic bacteria on erupted teeth when it reappears in saliva as opposed to topically strengthening enamel?
Another theory from the mid-20th Century is that fluoride delays the growth of teeth. This is not admitted to by pro-fluoridation mythologists. Yet ample research exists to show that there is a delay in primary tooth eruption when an infant and young child ingests fluoride. Younger teeth at the age five oral health examination means they have had shorter erupted time to become decayed. So, it’s not the delusional decay-preventing mechanism of fluoride but the delay in eruption caused by fluoride which makes fluoride seem like a magic bullet. Delay in eruption might seem like a neat idea to steer the teeth through the early years without becoming decayed, but anything which delays a child’s development artificially is to be proscribed.
It’s a paradox …
Even if we were to accept that fluoride strengthens parts of the immature enamel, it is also officially accepted that it damages the normal processes of enamel formation by stopping the clearance of protein in the developing enamel matrix such that the matrix cannot robustly form in the presence of the vestigial proteins. This results in dental fluorosis. How can fluoride strengthen enamel and at the same time cause a disruption to the enamel matrix? Surely both cannot be possible?
When the post-eruptive fluorosed enamel comes into contact with decay-causing bacteria, those bacteria are capable of moving into the dentine underlying the damaged enamel. That allows staining of the enamel and the underlying dentine due to food dyes. Decay and mucky teeth are the inevitable outcomes.

Moderate dental fluorosis from p. 6 of “A community-based study of dental fluorosis in rural children”
Another problem with dental milk in Blackpool primary schools is that Dr Rajpura has not authorised an evaluation of the programme so he cannot possibly prove that it is working to stop decay. As highlighted above, evaluation trials have provided limited or low/moderate quality results.
… and a contradiction
There are warnings on the back of an American fluoride toothpaste carton urging parental supervision to avoid swallowing the toothpaste.
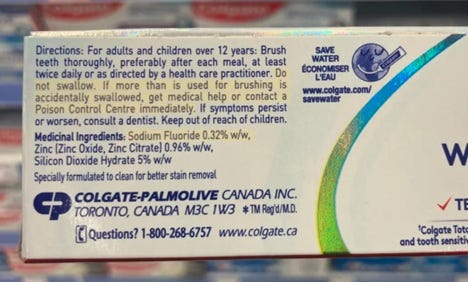
Courtesy of https://fluoridealert.org/news/69-reasons-to-oppose-adding-fluoride-to-water/
However, when drinking fluoridated milk, children are encouraged to swallow. The discovery of the enterosalivary route of fluoride through the body between the small intestine and salivary glands is not something which the general public is aware of. The circulating fluoride in saliva (and from swallowed fluoride toothpaste, food and water) is capable of disabling decay-causing bacteria but at what cost to the rest of the body if only a minute amount of fluoride reappears in the mouth via the salivary glands. Where does the rest of the fluoride go if it’s not in saliva, sweat, urine and faeces? It’s bad news for the body if fluoride bioaccumulates. That’s an essay for another time.
14th December 2025
Footnote: A small number of trials - including at least one reasonable double-blind trial (Stephen, 1984) and a randomized trial whose data were supplied to the Cochrane reviewers (Maslak 2004) - reported reductions in dental caries with fluoridated milk. However, the total RCT evidence base is small, many influential studies are older programmatic or pilot studies with methodological limitations, and at least one RCT (Maslak) was available only as abstract/unpublished full data. Systematic reviewers (Cochrane) therefore judge the overall evidence as limited / low–moderate quality despite generally favourable results. See also Cochrane: Fluoridated milk for preventing tooth decay, 2015, https://www.cochrane.org/evidence/CD003876_fluoridated-milk-preventing-tooth-decay